Introduction to Diagnostic Medical Parasitology
Essentials
Leishmaniae are protozoa belonging to the family Trypanosomatidae. On clinical grounds, they have been divided into three major groups: cutaneous, mucocutaneous and visceral. Visceral leishmaniasis is caused by intracellular protozoa of the Leishmania donovani complex and is transmitted by sandflies.
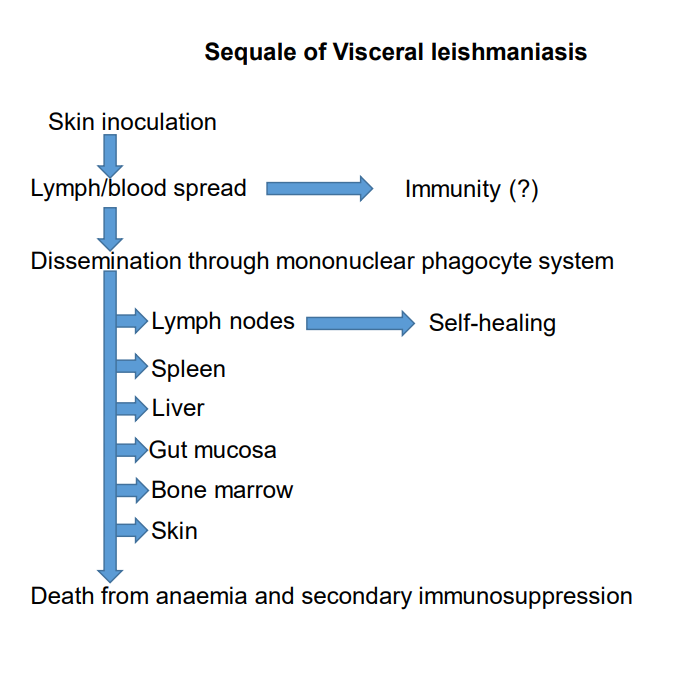
Parasites (promastigote forms) inoculated by the vector invade macrophages by induced phagocytosis. In a slowly progressive disease, spleen, liver, bone marrow and lymph nodes become infected. The disease is often fatal.

Epidemiology
- Visceral leishmaniasis is caused by members of the L. donovani complex:
L. d. donovani: in East India and northern and East Africa
L. d. infantum: in the Middle East and the Mediterranean region - Most species are anthropo-zoonotic, with dogs as an important reservoir
- Transmission by sandflies. Exceptionally, transmission from person to person by blood transfusion, transplants or sexual contact.
Pathology
- Amastigotes infect, survive and multiply in macrophages in many organs which are severely damaged
Clinical Findings
Many symptoms
- Prolonged fever, persistent and irregular
- Hepatosplenomegaly
- Lymphadenopathy
- Anaemia
- Leucopaenia
- Thrombocytopaenia
- General weakness
- The principal signs of visceral leishmaniasis are an enlarged spleen and prolonged irregular fever. Other signs are weight loss, pallor, an enlarged liver, enlarged lymph nodes, anaemia, cough and diarrhoea.
Diagnosis
Diagnostic methods
Parasitological diagnosis
Only rarely can amastigotes be demonstrated in buffy coat preparations from peripheral blood. Biopsies of spleen (risky!), liver, lymph node or bone marrow (sternum) have to be taken and stained for the detection of amastigote parasites.
Biopsies can be put into culture medium in which amastigotes transform to promastigotes and multiply.
Molecular diagnosis
Highly sensitive and specific nested PCR and real-time PCR methods have been developed to detect DNA in bone marrow or in biopsies. In underlying immunal suppression peripheral blood would be sufficient. Molecular methods are more sensitive than microscopy.
Serological detection
Method: IFAT
Note: In the case of a successful therapy, a decrease in titers can be observed in approximately 70% of patients two months after the end of treatment. Serological detection of cutaneous leishmaniasis is only occasionally achieved. PCR or in vitro culture are alternative methods recommended for diagnosis.
Diagnostic strategies
- To diagnose a symptomatic case
If a case is suspected from clinical findings, the detection of circulating antibodies is the next diagnostic choice. Confirmation of the diagnosis is then done by PCR or if this is not available, by microscopy.
- To screen an exposed population
For epidemiological studies, the direct agglutination test (DAT) is a convenient choice for screening.
Prevention and control
- Protection against bites by infected sandflies (clothing and repellents)
- Use of fine-meshed mosquito nets