Introduction to Diagnostic Medical Parasitology
Hookworm disease
Ancylostoma duodenale, Necator americanus
Essentials


Epidemiology
- Hookworm infections are distributed all over the world in warm and humid regions (conditions which are needed for larval development)
- In the past, hookworm disease was a threat during tunnel constructions (e.g. St. Gotthard, where hookworms were detected for the first time!) or in miners in Europe
- Ancylostoma duodenale is mainly found in southern Europe, northern Africa, the Middle East, India, China and the Far East
- Necator americanus prevails in South-East Asia, most of tropical Africa and North and South America, but is also found together with Ancylostoma in the Far East, India and South-East Asia
- Intensity of infection increases in childhood then levels off or declines in adults (sign of partial immunity)
- Humans are the only definitive host


Pathology
- There is damage (minor haemorrhage, inflammation, oedema) by the invading larvae in the skin and in the lung as a consequence of their migration
- Attachment of adult worms provokes haemorrhage and ulcerations in the small intestine
- Hookworms feed continuously on blood which causes blood loss in the host and may result in hypochromic microcytic anaemia.
Clinical Findings
- Characteristic cutaneous lesions (“ground itch”) by larval penetration and secondary bacterial infections after scratching
- Pulmonary symptoms (1 to 2 weeks after infection) with dry cough, asthmatic wheezing, tracheitis and fever may occur during the lung migration phase
- Gastrointestinal symptoms may be absent or may lead to a variety of symptoms (e.g. anorexia, flatulence, abdominal discomfort and diarrhoea)
- Heavy and chronic hookworm infections lead to anaemia accompanied by other manifestations (like apathy, fatigue, palpitation)
- In schoolchildren heavy infections may have serious consequences (retarded growth, delay in puberty and eventually mental retardation)
Diagnosis
Diagnostic methods
Parasitological diagnosis
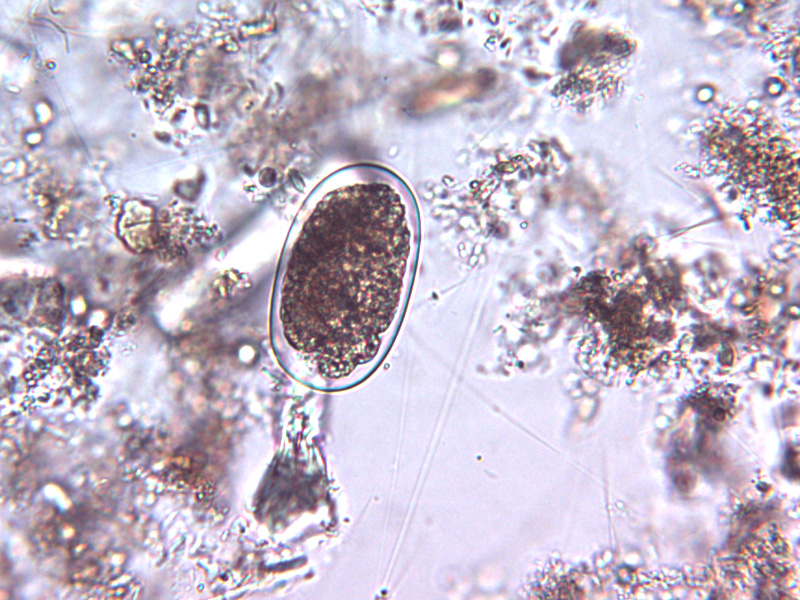
Ova can be easily recovered from fresh stools using direct smears or concentration methods.
In older unpreserved stool samples, rhabditiform larvae can be detected and have to be distinguished from Strongyloides. Hookworm larvae have a long, Strongyloides, a very short buccal cavity!
Molecular diagnosis
Molecular tools in evaluation process
Antigen detection
No tests available
Antibody detection
Is of no diagnostic value
Diagnostic strategies
Besides microscopic examinations, no special diagnostic strategy is required!
Prevention and control
- To prevent hookworm infections, contact of bare skin with contaminated soil should be avoided.
Proposed measures: wearing shoes, reduce faecal contamination of soil by sanitation (installation of latrines, personal hygiene). - Health education is essential to control hookworm disease
- Mass treatment (has no effect if no change in sanitation and hygiene!)