Introduction to Diagnostic Medical Parasitology
Essentials
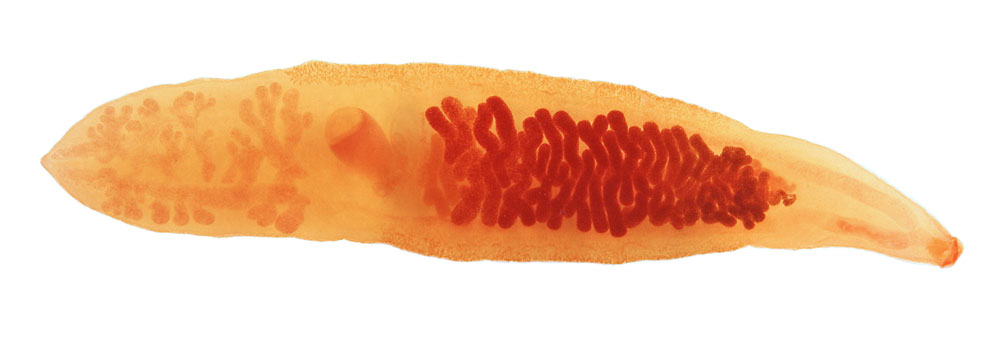
Clonorchiasis is due to an infection with the small liver fluke Clonorchis sinensis (Opisthorchis sinensis). Adult flukes (with a length of up to 2.5 cm) inhabit the distal bile ducts.
The fully developed eggs are passed with the faeces. For further development of the miracidium, eggs have to be eaten by the first intermediate host, a water snail. In the first intermediate host, thousands of cercariae are produced which have to find the secondary intermediate host where they encyst in the superficial tissue and become metacercariae. Fish-eating animals and humans become infected by eating raw fish. The prepatent period - from infection until first eggs are found in the faeces - is about a month. To complete this, life cycles within three hosts needs at least 3 months.
Epidemiology
- Clonorchiasis is highly endemic in south-east China, Vietnam, Laos, Cambodia (Mekong river delta). It also occurs in Japan, Taiwan and Korea.
- People are infected by eating raw or undercooked freshwater fish containing encysted larvae
- Children are more frequently infected than adults
- Fish-eating domestic but also wild animals serve as reservoir hosts


Pathology
- No early liver damage since young flukes ascend the biliary tree from the duodenum
- Severity of the disease depends on the worm burden
- Pathology is caused by mechanical damage and also by toxic effects of parasitic metabolites
- The gall bladder might be enlarged in heavy infections
- In heavy chronic infections, one might find fibrosis of the bile duct and periductal tissues
Clinical Findings
- Most infections are asymptomatic
- Early symptoms are very rare; in chronic infections, symptoms vary: weakness, anorexia, diarrhoea, light fever, liver symptoms and epigastric pain
- Complications after bile duct stenosis are rare
Diagnosis
Diagnostic methods
Parasitological diagnosis
Diagnosis is proven by finding the characteristic eggs in faeces or in duodenal fluid (by duodenal aspiration or with the “string test”).
Multiple samples and concentration methods improve sensitivity in light infections!
Molecular diagnosis
First attempts to detect and differentiate DNA from Asian liver flukes (C. sinensis, O. viverrini and O. felineus) in faecal samples using specific primers
Antigen detection
No tests developed so far
Antibody detection
Serological tests using crude worm antigens have low specificities (cross-reactivity with other trematode infections).
A better specificity can be reached using recombinant or purified antigens (e.g. cysteine proteinase or excretory/secretory antigens). However, there is a loss in sensitivity.
Diagnostic strategies
- Screening populations to assess prevalence
Perform a cross-sectional study analysing fixed stool specimens with a concentration method (preferably after sedimentation).
As an alternative screening method, serology could be used (if multiple trematode species are not prevalent!)
- Detecting clonorchiasis in exposed individuals
Examine one or multiple fresh stool specimens for ova after concentration

Prevention and control
- In endemic areas, people should be educated about the dangers of eating raw or undercooked fish (by freezing fish, metacercariae are killed!)
- Faeces should be disposed of in a sanitary way
- No night soil or animal waste should be deposited in fish ponds